In cataract
surgery, cloudy crystalline lens is removed and replaced by clear artificial
lens called intra-ocular lens. There are various methods for cataract
extraction and most recent and efficient one is phacoemulsification and
intra-ocular lens implantation1. In phacoemulsification, ultrasonic
vibrations are used to break the crystalline opaque lens into pieces which are
then removed by aspiration.
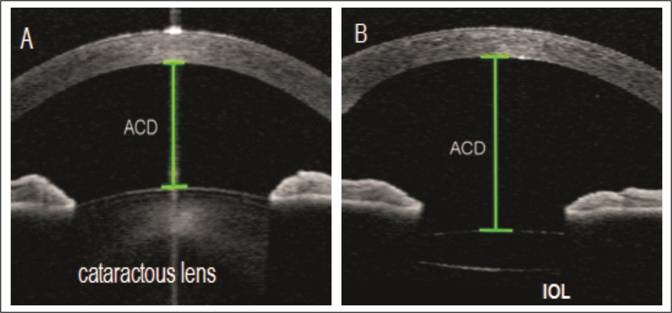
Cataract extraction and IOL implantation causes change in anterior
chamber configuration2 that includes an increase in anterior chamber
depth (ACD), increase in anterior chamber angle (ACA) withincrease in angle
depth and width. These changes in anterior chamber configuration ultimately
lead to fall in intra-ocular pressure3.
There are various methods to determine anterior chamber details that
include Gonioscopy for anterior chamber angle details, ultrasound Biomicroscopy
(UBM), that gives high resolution images of anterior chamber4,5,6 and
anterior segment OCT.
The most recent one is anterior segment optical coherence
tomography(AS-OCT) that uses light of longer wavelength and is superior being
non-contact and non-invasive, having less inter-observer and intra- observer
variability, rapid and easy to perform, providing efficient storage capacity
for images that can be visualized at any time7.
The rationale of our study was to study how
much angle is widened after cataract extraction with resultant decrease in
intra-ocular pressure (IOP) in our local population. The purpose of this study
is the quantitative measurement of change in anterior chamber angle depth and
width after uneventful phacoemulsification and intra-ocular lens implantation
in normal population using anterior segment optical coherence tomography
(AS-OCT).
MATERIAL AND METHODS
After approval from hospital ethical
committee, a written informed consent with demographic information was
collected from each patient before participating in this study. Patients of
both genders, between 50-70 years of age, with senile cataract, having
uneventful cataract surgery were randomly included in this study. Glaucoma
patients, patients with previous intra-ocular surgery and with optic nerve or
retinal dysfunction were excluded from this study. This study included 82
patients(sample size was calculated using formula  and values taken from Junejo, et al.,2016 study). It was conducted at eye
department of DHQ-Teaching Hospital Gujranwala from January 2018 to June 2018.
and values taken from Junejo, et al.,2016 study). It was conducted at eye
department of DHQ-Teaching Hospital Gujranwala from January 2018 to June 2018.
All patients underwent routine ophthalmic examination including unaided
visual acuity (UVA), visual acuity with pinhole (PH), best corrected visual
acuity (BCVA), Slit lamp Biomicroscopy and Fundus evaluation. Biometry of the respected
eye was done to determine axial length and IOL power. Gonioscopy was done by
experienced examiner in dark to exclude patients with angle closure glaucoma. Goldmann
applanation tonometry and anterior segment optical coherence tomography
(Optovue; Model iVue 500) of respected eye was done pre-operatively and 2 days
post-operatively in non-dilated eye under dark conditions. While performing
AS-OCT the patient was asked to sit comfortably with forehead touching the
forehead rest and fixate on the green indicator. Focusing was done manually. One
examiner, masked to the results of clinical findings performed AS-OCT in
temporal quadrant of respected eye under standardized dark conditions. Scans
were manually centered on pupil and auto-adjusted to obtain best quality
images. One best image was selected among all with no motion or artifact due to
eyelid movements. These images were finally
processed using customized software by the same experienced observer. The only
input of examiner was to determine the location of the scleral spurs. The
algorithm then automatically calculated the anterior segment parameters. Among
all parameters, Trabecular iris angle (TIA) and Angle opening distance at 500
(AOD-500) were included in this study.
Two surgeons performed all cataract surgeries using phacoemulsification
under retro-bulbar anaesthesia with 1% lignocaine and 0.5% bupivacaine followed
by 10 minutes of external ocular massage. Temporalclear corneal incision was
given that was not sutured at the end of surgery. Uneventful
phacoemulsification and foldable IOL implantation was done. If accidently any
case met a per-op or post-op complication, then it was excluded from this
study. Patients were discharged on second post-op day after repeating IOP and
AS-OCT of respected eye.
Data was analyzed
using SPSS version 23.0. Results were expressed as mean ± SD and ranges. Comparison
between pre-operative and post-operative angle parameters was done using a
paired t-test. A P-value ≤ 0.05 was considered to be
statistically significant.
RESULTS
82 patients were
included in this study. Out of which 38 (46.3%) were female and 44 were male (53.7%).
Right eye was involved in 42 cases (51.2%) and left one in 40 cases (48.8%).
Average age noted was 60.7 ± 6.5 (range 50-70) years. 50 patients (61%) were
below 60 years of age and 32 patients (39%) were above 60 years of age.
|
Demographic
Variables |
Study Population(n=50) |
|
Age: Mean
± SD |
60.7±6.5 |
|
Gender Male/Female |
53.7%(44)/46.3%(38) |
|
Laterality: Right/Left |
51.2%(42)/48.8%(40) |
Ø Mean IOL power recorded was 22±3.2 with Range of 11-29.5 D and Mean Axial
length recorded was 23±1.2 with Range of 16.6-27.3 mm.
Fig. 1a: Axial length readings. X-axis showing no of pts. and y-axis showing Axial length in mm.
Fig. 1b: IOL power readings. X-axis showing no of pts. and y-axis showing IOL Power in Diopters.
Ø Only foldable intra-ocular lenses were being used during phaco surgery.
Various types of foldable IOL with their frequencies are given in following
table;
|
Types eeof Intraocular Cataract Lenses |
Frequency |
Percent |
|
Alcon |
7 |
8.5 |
|
BF |
16 |
19.5 |
|
Focus Force |
25 |
30.5 |
|
I-stream |
24 |
29.3 |
|
PhysIOL |
3 |
3.7 |
|
Zeiss |
7 |
8.5 |
|
Total |
82 |
100.0 |
Ø Mean Pre-op TIA recorded was 41.5 ± 8.7°
that widened to 48.6 ± 8.3°
post-operatively with significant p-value of 0.0001 (< 0.05).
|
Trabecular
Iris Angle (TIA) |
Mean |
n |
Std.
Deviation |
p-value |
|
Pre-op TIA |
41.5 |
82 |
8.7 |
0.0001 |
|
Post-op TIA |
48.6 |
82 |
8.3 |
Fig.2: Pre and post op TIA. X-axis showing no of pts. and y-axis showing TIA in°
Ø Mean pre-op Angle opening distance (AOD-500 μm) recorded was 447.5 ± 149.8 μm
that increased to 609.5±169.8μm
post-operatively with significant p-value of 0.0002 (< 0.05).
|
Anterior Chamber (AOD-500 μm) |
Mean |
n |
Std. Deviation |
p-value |
|
Pre-op
(AOD-500μm) |
447.5 |
82 |
149.8 |
0.0002 |
|
Post-op
(AOD-500μm) |
609.5 |
82 |
169.8 |
Fig.3: Pre and post op AOD. X-axis showing no of pts. and y-axis showing AOD-500 in μm.
Ø Mean Pre-op IOP recorded using Goldmann Applanation Tonometer was 16.8 ± 2.8
mmHg that declined to 15.1 ± 2.9 mmHg post-operatively with significant p-value
of 0.00001 (< 0.05).
|
Intraocular Pressure (IOP) |
Mean |
n |
Std.
Deviation |
p-value |
|
Pre-IOP |
16.8 |
82 |
2.8 |
0.00001 |
|
Post-IOP |
15.1 |
82 |
2.9 |
Fig.4: Pre and post op IOP. X-axis showing no of pts. and y-axis showing IOP in mmHg.
DISCUSSION
This study is based on a simple question,”
Does cataract extraction improve aqueous outflow or not?” To prove this, we
conducted this study. For which, we included patients with senile cataract
having uneventful cataract surgery while excluding glaucoma patients and
patients with previous intra-ocular surgery to minimize confounding factor.
Anterior chamber angle parameters were being studied pre and post-operatively
using AS-OCT.
Various studies have been
done in glaucomatous as well as non-glaucomatous eyes to determine changes in
anterior chamber configuration after cataract surgery. In glaucoma patients, it
makes the basis for clear lens extraction and IOL implantation to reduce
intra-ocular pressure (IOP)8.
In a study published by Kim
et al 11 eyes of 11 patients with angle closure glaucoma (ACG) and 12 eyes of
12 patients with open angle glaucoma (OAG) were included. The results showed
that central ACD and angle parameters as measured by AS-OCT increased
significantly in eyes with glaucoma (p < 0.05) after cataract extraction.
Before surgery, mean central ACD in the ACG group was approximately 1.0 mm
smaller than that in the OAG group (p < 0.001). After surgery, mean ACD of
the ACG group was still significantly smaller than that of the OAG group. In
the ACG group, postoperative IOP at the final visit was significantly lower
than preoperative IOP (p = 0.018)9.
Another study compared the
role of cataract surgery in normal population with only cataract and in
patients with both cataract and normal tension glaucoma (NTG) using swept
source-optical coherence tomography (SS-OCT). And they concluded that angle
parameters remarkably increased in both groups but IOP changes were only
statistically significant in patients with normal tension glaucoma10.
A study published by Junejo
et al showed the effect of uneventful cataract surgery on anterior chamber
depth (ACD) using ultrasonography A-Scan in 74 healthy eyes. Results showed
that the mean ACD after 1 day of cataract surgery was 3.46 ± 0.44, mm after 1
week of surgery was 3.64 ± 0.46, mm and after 1 month of surgery was 3.81 ±
0.46. mm Significant increase of 0.73 ± 0.58 mm (p < 0.0001) in the mean ACD
was seen after 1 month of uneventful cataract surgery11.
There are various angle parameters which
include
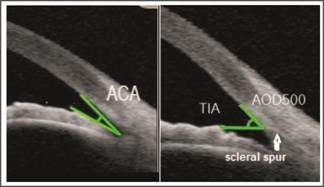
Fig. 1: Anterior
chamber angle (ACA) is the
angle between the iris anterior surface and that of the posterior corneal
surface with its apex in the angle recess. Trabecular
Iris angle (TIA) is the angle that is measured with its apex in the scleral
spur and the arms500 µm from the scleral spur passing through a point on the
trabecular meshwork and a perpendicular point on the iris.
ACA, TIA, AOD-500,
AOD-750, TISA-500, TISA-750 which are being discussed in following paragraph
along with diagrammatic illustrations.
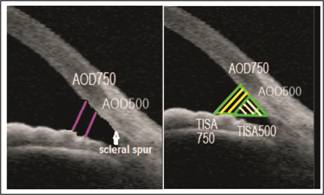
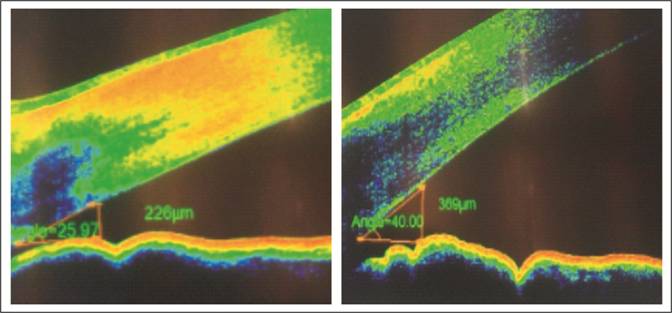
Fig 2: Angle
opening distance at 500μm
(AOD-500) and 750μm
(AOD-750) is the distance from the corneal endothelium to the anterior surface of iris
just perpendicular to a line drawn along the trabecular meshwork at 500 and
750µm from scleral spur. Trabecular-iris
space areas (TISA) defined as the areas bounded by the corneal endothelium,
trabecular meshwork, and anterior iris surface out to a distance of 500 µm or
750 µm from the scleral spur.
In this study, we included Trabecular iris
angle (TIA) and Angle opening distance at 500μm
(AOD500). Both of these actually specify ACA depth and width and are
standardized as well. Reason not to include ACA is that it was difficult to
identify proper angle recess in many patients and thus it can lead to reduced
study sensitivity. It is important to note that ACA depth is different from
Anterior chamber depth (ACD) and this study doesn’t include ACD that is the
distance from corneal endothelium at the center of cornea to the anterior
surface of lens12. Though previous studies included ACD change that
can be well explained on this fact that thick cataractous lens is replaced with
a thin intra-ocular lens that will ultimately deepen the AC13. Another
limitation for this parameter is that it includes some portion of posterior
chamber when measured in eyes with intra-ocular lens while we are only
concerned about anterior chamber.
It was very surprising to
note that after cataract surgery, anterior chamber angle depth and width
increased when examined via Anterior segment OCT(AS-OCT) giving quantitative
proof by measuring TIA and AOD500 pre
and post-operatively as documented in some previous studies as well. In this study, we included surgeries with only foldable intra-ocular
lenses to eliminate confounding factor, single piece IOL’s with an optic
diameter of 6.0